|
|
|
|
|
|
|

|
| MTM Newsletter |
N° 4 - July/August 2013 | |
|
|
|
| |
|
|
| |
|
|
| |
|
|
|
Laboratory News
|
 Notes about quality control, plausibility checks and a plea for improved cooperation Notes about quality control, plausibility checks and a plea for improved cooperation
|
For metal testing, our report delivery time is, most likely, the best in the industry. Occasionally, data release is put on hold because extreme values are not plausible i.e. inadequate sample information requires us to fully repeat sample testing. For example, if the submission sheet informs us that the patient is on lithium or iodine therapy, this useful information is appreciated by the quality control people. If the information is not given, we automatically repeat the test, which will require time. Data won’t be released until quality control assurance is completed.
Repeat analysis is often required for the following elements. If we had sufficient information, we could deliver results quicker, would need to repeat fewer tests, saving energy and other costs. If appropriate, please notify us about:
|
- Lithium-Therapy
- Contrasting agents such as Gadolinium, Iodine, Cobalt, Barium etc.
- Oral intake of Iodine
- Use of Boric acid in urine collection container. (Not needed for urine metal tests)
|
We also appreciate your assistance with the following:
|
- Urine: We provide metal-free urine tubes and protection containers with an absorption lining. Unfortunately, we sometimes receive urine samples
not in the 15ml metal-free tube but in the larger, absorption-lined protection container. This causes contamination; high aluminum values can be expected!
- Hair: We often receive chemically-treated hair. If visual distinction is possible, we reject such samples. But the problem is not always obvious optically, before sample preparation and analysis has started. Please be advised that chemical treatment of hair (coloring, perming, bleaching etc.) falsely elevates metal values. It is impossible to properly validate such results.
|
Fees
|
When we receive one baseline urine and provocation urine from the same patient on the same day, we perform a metal test on each sample, meaning there are two charges. If both samples are received at the laboratory on the same day, we provide a 10% discount from the total sum.
|
Reference range vs. Orientation range
|
Our reports show
reference ranges as provided by environmental agencies. The German Umweltbundesamt (UBA) and the CCC (Center for Disease Control) lowered ranges for toxic metals such as lead. The UBA defines a reference range as ‘the range for a chemical in a human specimen that has been analytically defined from a specific (EBB note: so-called healthy) population.’ For more on statistical evaluation see
O.M. Poulsen, E. Holst
and J.M. Christensen: A supplement to the approved IFCC
Recommendation on the theory of reference values. In: Pure & Appl.
Chem., Vol. 69, No. 7, pp. 1601-1611, 1997
The US Center for Disease Control (CDC) states that a “reference range value is based on the 97.5th percentile of the 2007-2010 National Health and Nutrition Examination Survey’s (NHANES). CDC will update reference range value periodically using the two most recent NHANES surveys.
|
The most common toxins agencies provide reference ranges for blood and urine, but the urine ranges explicitly and
only apply for baseline urines.
EDTA, DMSA and DMPS are chemical substances with strong metal binding abilities. For example, a urine sample collected after DMPS provocation will show high copper levels, even if the patient is borderline deficient. Similarly, EDTA will bind iron or calcium. To compare provocation urine values with borderline reference ranges is misleading.
For this reason, we developed Orientation Ranges (OR). The following table shows ORs for lead (Pb) as applicable for the different chelating agents, indicating that EDTA is best for lead binding.
|
|
|
Baseline Reference Range
|
DMSA
Orientation Range
|
DMPS
Orientation Range
|
EDTA
Orientation Range
|
|
Lead
|
5
|
10
|
12
|
22
|
Values in mcg/g Creatinine |
|
|
To generate provocation urine reports with the appropriate OR, we appreciate receiving specific information regarding type and amount of chelation agent used. In addition, we appreciate being informed about the urine collection time, which influences metal output.
If no information is provided, reports are generated
without the orientation range i.e. test values are compared to the baseline reference range.
If you don’t want us to use ORs, please let us know (via phone, fax or e-mail). However, it would help us and our validation process, if you provide us with the information as outlined above.
Test values in mcg/g - mg/g Creatinine or mcg/l - mg/l.
Our urine reports list test values in mg/g creatinine i.e. mcg/g creatinine. By using the creatinine concentration as a mathematical factor, diuresis effects are considered. To list test values in mcg i.e. mg/l is only useful when the amount of urine collected is precise, and that is usually not the case, resulting in misleading information.
|
Insurance Information
|
The ‚Medical Necessity’ of Metal Testing
If a metal intoxication is suspected through patient evaluation and history taking, it is the physician’s responsibility to confirm or refute it. The following statements about causes, diagnosis and treatment are from
Medical Dictionary and refer to heavy metal poisoning. Without proper diagnostics, the differentiation between acute and chronic overexposure may be difficult. Timing can be critical.
Causes and symptoms
Symptoms will vary, depending on the nature and the quantity of the heavy metal ingested (or otherwise exposed to). Among the complaints most often listed are nausea, vomiting, diarrhea, stomach pain, headache, sweating, and a metallic taste in the mouth.
Diagnosis
Heavy metal poisoning or overexposure may be detected using blood and urine tests, hair and tissue analysis, or x ray. The diagnosis is often difficult to make, however, because many of the early symptoms of heavy metal poisoning or long-term overexposure are nonspecific. The doctor should take a thorough patient history with particular emphasis on the patient's occupation. Note: an insufficiently treated acute metal poisoning will, in time, turn into a chronic intoxication.
Treatment
When heavy metal poisoning is suspected, it is important to begin treatment as soon as possible to minimize long-term damage to the patient's nervous system and digestive tract.
|
New Tests
|
As of now we test Porphyrines in Urine and Vitamin D.
Porphyrines
Porphyrins are organic compounds, one of them being hemoglobin, the protein in the red blood cells which carries oxygen in the blood. Porphyrins can be best measured in the urine.
Read more on our Website:
http://www.microtraceminerals.com/en/diagnostic-humans/urine/porphyrins-urine
Vitamin D
Vitamin D is referred to as a fat-soluble vitamin when in fact it is a pre-hormone, necessary for many body functions. It is stored in fatty tissue for longer periods of time, meaning that daily intake, in most cases is not needed.
More Information also on our Website:
http://www.microtraceminerals.com/en/diagnostic-humans/micronutrients-and-vitamins/vitamin-d
|
New Newsletter Format
|
To make our newsletter easier to read we have introduced a new newsletter format, with color codes.
|
|
Laboratory News / MTM News
 Information’s about Workshops and Conferences Information’s about Workshops and Conferences
 Information’s about actual Studies and Analyses Information’s about actual Studies and Analyses
|
|
We hope you enjoy it.
Please tell us your valued opinion:
http://www.microtraceminerals.com/en/about-us/testimonial
|
| |
| |
|
|
| |
|
|
|
Medical Workshops and Conferences
|
International Conferences & Workshops 2013-2014
|
| 10/09/2013 - 10/11/2013 |
Medical Challenges +
Chelation (ICIM)
Columbus, Ohio, USA
(English) |
|
| 10/26/2013 |
Scientific Conference for toxicology of heavy metals
Orléans,
France (French / English) |
Dr. M. Verheyen |
| 10/30/2013 - 11/03/2013 |
47. Medical
Week
Baden-Baden (KMT)
Baden-Baden (German /
English) |
|
| 11/08/2013 - 11/10/2013 |
14. Memminger Gesundheitstage
Memmingen (German) |
|
| 03/15/2014 |
Physicians Workshop
Nuremberg (German) |
Dr. T. Fischer |
| 03/29/2014 |
Natural Health Professional Workshop
Nuremberg (German) |
|
| 05/01/2014 - 05/03/2014 |
Chelation Conference
Sao Paulo,
Brazil
(English / Portuguese) |
Prof. Dr. Efrain Olszewer |
|
Details under:
http://www.microtraceminerals.com/en/workshops
|
IBCMT (International Board of Clinical Metal Toxicology) Certification
|
As of now, the IBCMT written examination can be done online. To successfully qualify for IBCMT certification, it is necessary to study the IBCMT Textbook of Clinical Metal Toxicology.
More informations on the
IBCMT Homepage.
|
| |
| |
|
|
| |
|
|
|
|
|
Studies and Analyses
|
TACT Studie (Trial to Assess Chelation Therapy)
|
This long awaited study with the objective to determine if an EDTA-based chelation regimen reduces cardiovascular events has been completed and published.
For this double-blind, placebo-controlled, 2 × 2 factorial randomized trial 1708 patients aged 50 years or older who had experienced a myocardial infarction (MI) at least 6 weeks prior and had serum creatinine levels of 2.0 mg/dL or less. Participants were recruited at 134 US and Canadian sites. Enrollment began in September 2003 and follow-up took place until October 2011 (median, 55 months). Two hundred eighty-nine patients (17% of total; n=115 in the EDTA group and n=174 in the placebo group) withdrew consent during the trial.
Patients were randomized to receive 40 infusions of a 500-mL chelation solution (3 g of disodium EDTA, 7 g of ascorbate, B vitamins, electrolytes, procaine, and heparin) (n=839) vs. placebo (n=869) and an oral vitamin-mineral regimen vs. an oral placebo. Infusions were administered weekly for 30 weeks, followed by 10 infusions 2 to 8 weeks apart. Fifteen percent discontinued infusions (n=38 [16%] in the chelation group and n=41 [15%] in the placebo group) because of adverse events.
Conclusions and Relevance: Among stable patients with a history of MI, use of an intravenous chelation regimen with disodium EDTA, compared with placebo, modestly reduced the risk of adverse cardiovascular outcomes, many of which were revascularization procedures. These results provide evidence to guide further research.
However, the researchers also conclude that the results do not fully support the routine use of chelation therapy for treatment of patients who have had an MI. (Note: no attention was paid to the anti-inflammatory effects of EDTA chelation therapy.)
For more detailed information see:
http://jama.jamanetwork.com/article.aspx?articleid=1672238
|
Information about Calcium- and Copper binding of NaCaEDTA, NaMgEDTA, DMPS & DMSA
|
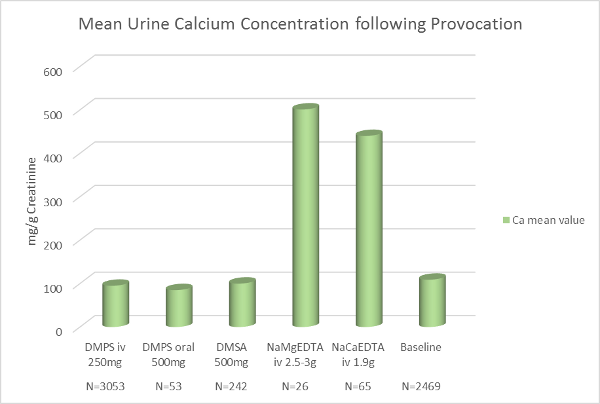
Calcium (Ca)
We compared the mean value concentration for calcium following the application of the chelating agents NaCaEDTA and NaMgEDTA with other chelating substances. As expected, the intravenous application of NaCaEDTA as well as NaMgEDTA resulted in a high urinary calcium excretion.
Note:
Through the i.v. application of NaCaEDTA, high amounts of calcium are injected directly into the bloodstream. With the administration of NaMgEDTA we do not add any calcium, but bind serum and otherwise available calcium. Consequently, NaMgEDTA is indicated in the treatment of Hypercalcemia. As has been noted decades ago, NaMgEDTA has the ability to potentially prevent and possible ‘dissolve’ calcium deposits. For the treatment of these cases, CaNaEDTA is contraindicated.
Diagram 1 shows the urinary calcium excretion following NaCaEDTA and NaMgEDTA. It also indicates that the chelating agents DMPS und DMSA do not noticeably affect calcium. |
|
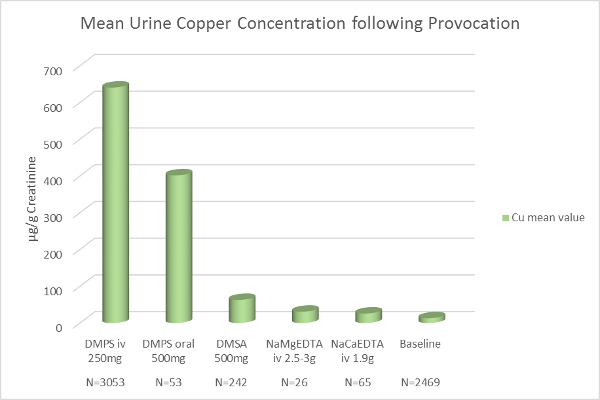
Copper (Cu)
Diagram 2 indicates that both forms of DMPS (intravenously or orally applied) have a significant copper binding ability. The urinary copper excretion following oral DMSA is slightly higher than that of the intravenously applied EDTAs, but is comparatively unremarkable. |
|
Note:
From the above information, we can apply the plausibility check. For example, if a provocation test shows a urine copper value of 300mcg/g creatinine and the submission sheet lists the sample as an EDTA provocation test, we can assume an error in information. Therefore, we inform the appropriate office or doctor or make a note on the report. |
| |
| |
| |
|
|
|
|
|
|
|
We wish you a pleasant and relaxing summer.
Your
E.Blaurock-Busch and Team
|
|
|
|
| |
|
|
| |
|
|
|